

Immune Checkpoint Inhibitors & CAR T-Cell Therapy
The human immune system has the remarkable ability to distinguish self from non-self and to eliminate abnormal cells, including cancer. However, tumors evolve sophisticated mechanisms to evade immune detection and destruction. Immune Checkpoint Inhibitors are monoclonal antibodies that block these evasion mechanisms, "releasing the brakes" on the immune system and enabling it to attack cancer cells. Drugs like pembrolizumab (Keytruda), nivolumab (Opdivo), and ipilimumab (Yervoy) target checkpoint proteins such as PD-1, PD-L1, and CTLA-4, and have become standard treatments for melanoma, lung cancer, kidney cancer, and many others. Complementing checkpoint inhibitors is CAR T-Cell Therapy, a form of adoptive cell transfer where a patient's own T cells are genetically engineered to express a chimeric antigen receptor (CAR) that recognizes and kills cancer cells. Unlike checkpoint inhibitors, which work for many cancer types, CAR T-cell therapy is currently approved primarily for hematologic malignancies—B-cell acute lymphoblastic leukemia, non-Hodgkin lymphoma, and multiple myeloma. For oncologists, immunologists, and cancer researchers, the detailed analysis on Immune Checkpoint Inhibitors provides essential insights.
H2: Mechanisms of Action
Immune Checkpoint Inhibitors target proteins that normally regulate T-cell activation. Under physiological conditions, checkpoints prevent autoimmune disease by limiting T-cell responses. Cancer cells exploit these checkpoints to evade immunity. PD-1 (programmed cell death protein-1) is expressed on activated T cells; its ligands PD-L1 and PD-L2 are expressed on many cancers. When PD-1 binds PD-L1, T-cell activation is suppressed. Anti-PD-1 antibodies (pembrolizumab, nivolumab) block this interaction, restoring T-cell function. CTLA-4 (cytotoxic T-lymphocyte-associated protein-4) competes with CD28 for binding to B7 molecules on antigen-presenting cells; CTLA-4 activation suppresses early T-cell activation. Ipilimumab blocks CTLA-4, enhancing T-cell priming.
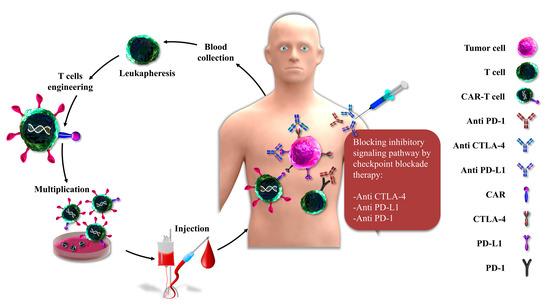
CAR T-Cell Therapy takes a different approach. T cells are collected from the patient by leukapheresis, then genetically modified using a viral vector (lentivirus or retrovirus) to express a CAR—a synthetic receptor that combines an antibody-like recognition domain (single-chain variable fragment, scFv) with T-cell signaling domains (CD3ζ and costimulatory domains like CD28 or 4-1BB). The CAR recognizes a specific antigen on cancer cells (e.g., CD19 on B cells, BCMA on plasma cells) independently of MHC presentation. After expansion in culture (2-3 weeks), the CAR T cells are infused back into the patient, where they proliferate and kill antigen-expressing cancer cells.
Both Immune Checkpoint Inhibitors and CAR T-Cell Therapy can cause immune-related adverse events (irAEs). Checkpoint inhibitors cause dermatitis, colitis, hepatitis, pneumonitis, and endocrinopathies (hypophysitis, thyroiditis, adrenalitis). CAR T-cell therapy causes cytokine release syndrome (CRS) —fever, hypotension, hypoxia—and immune effector cell-associated neurotoxicity syndrome (ICANS)—confusion, aphasia, seizures. Both require specialized management.
H2: Clinical Indications
Immune Checkpoint Inhibitors are approved for over 15 cancer types. Melanoma: pembrolizumab, nivolumab, ipilimumab (first-line, alone or combination). Non-small cell lung cancer: pembrolizumab first-line for PD-L1≥50%, or in combination with chemotherapy regardless of PD-L1; nivolumab second-line. Renal cell carcinoma: nivolumab plus ipilimumab first-line. Hodgkin lymphoma: pembrolizumab, nivolumab after relapse. Head and neck squamous cell carcinoma: pembrolizumab, nivolumab. Urothelial carcinoma, gastric cancer, esophageal cancer, cervical cancer, hepatocellular carcinoma, Merkel cell carcinoma, colorectal cancer (MSI-high), endometrial cancer (MSI-high). PD-L1 expression by immunohistochemistry predicts response for some indications but not others.
CAR T-Cell Therapy indications: B-cell acute lymphoblastic leukemia (B-ALL)—tisagenlecleucel (Kymriah) for children and young adults up to age 25 with relapsed/refractory disease. Diffuse large B-cell lymphoma (DLBCL)—axicabtagene ciloleucel (Yescarta), tisagenlecleucel, lisocabtagene maraleucel (Breyanzi) for relapsed/refractory after two or more lines. Multiple myeloma—idecabtagene vicleucel (Abecma), ciltacabtagene autoleucel (Carvykti) for relapsed/refractory after four or more lines. Mantle cell lymphoma—brexucabtagene autoleucel (Tecartus). Follicular lymphoma—axicabtagene ciloleucel. CAR T-cell therapy is not approved for solid tumors due to target antigen heterogeneity, immunosuppressive tumor microenvironment, and on-target off-tumor toxicity.
H2: Response Rates and Durability
Immune Checkpoint Inhibitors have variable response rates. Melanoma: 40-60% response to anti-PD-1 alone, 50-70% to anti-PD-1 plus anti-CTLA-4. Lung cancer (PD-L1≥50%): 45% response to pembrolizumab. Hodgkin lymphoma: 70-80% response to nivolumab or pembrolizumab. Durable responses (lasting years) occur in a subset of patients—the "tail of the plateau" on Kaplan-Meier curves. Some patients achieve complete remission and remain disease-free after stopping therapy. Others progress after initial response (acquired resistance) or never respond (primary resistance). Biomarkers beyond PD-L1 (tumor mutational burden, microsatellite instability, mismatch repair deficiency) identify patients more likely to respond.
CAR T-Cell Therapy response rates in hematologic malignancies are dramatic. B-ALL: 80-90% complete remission in relapsed/refractory patients who had exhausted other options. DLBCL: 50-60% complete remission, 70-80% overall response. Multiple myeloma: 70-80% overall response with ide-cel, 95% with cilta-cel (though follow-up shorter). Durability varies: 30-50% of DLBCL patients remain progression-free at 2 years; 50-70% of B-ALL patients relapse within 12 months (often with CD19-negative escape variants). The tumor microenvironment and CAR T-cell persistence affect durability.
H2: Future Directions
The future of CAR T-Cell Therapy includes allogeneic ("off-the-shelf") CAR T cells from healthy donors (reducing cost and wait time), dual-targeting CARs (CD19/CD20, CD19/CD22) to prevent antigen escape, CARs for solid tumors (targeting mesothelin, HER2, GD2, GPC3), and safety switches (inducible suicide genes) to manage toxicity. For Immune Checkpoint Inhibitors, novel targets (LAG-3, TIGIT, TIM-3, VISTA) are in development, as well as combination with other immunotherapies (CAR T cells, cancer vaccines) and conventional therapies (chemotherapy, radiation, targeted therapy). For oncologists and cancer researchers, the market research available on CAR T-Cell Therapy offers comprehensive guidance.
